Anorectal Malformation/ Imperforate Anus
Anorectal Malformations or Imperforate Anus is a pretty common congenital anomaly among neonates. Its reported incidence is 1 in 5000 live births. Considering the same incidence, our country must be having at least 40 to 50 thousand patients suffering from the same disease. These patients may have a huge variety of presentations. Their hole for potty may be completely absent, mislocated, opening into the Urinary bladder, or connecting with the urinary opening. So it is important to look into the exact diagnosis, where it might be leading.
Types of Anorectal Malformation:
Anorectal Malformation can present in a variety of ways in children. It is slightly different in both boys and girls.Among boys, it may be any of the following:
- Imperforate Anus without Fistula — Rectum is closed and does not open anywhere.
- Imperforate Anus with Recto-vesical Fistula — Rectum is abnormally opening into Urinary Bladder.
- Imperforate Anus with Recto-prostatic Fistula — Rectum is abnormally opening into Prostate.
- Imperforate Anus with Recto-Urethra Fistula — Rectum is abnormally opening into Urethra.
- Imperforate Anus with Perineal Fistula — Rectum is abnormally opening into Skin.
Among girls, it may be any of the following:
- Imperforate Anus without Fistula — Rectum is closed and does not open anywhere.
- Imperforate Anus with Recto-vesical Fistula — Rectum is abnormally opening into Urinary Bladder.
- Imperforate Anus with Recto-Vaginal Fistula — Rectum is abnormally opening into Vagina.
- Imperforate Anus with Recto-Vestibular Fistula — Rectum is abnormally opening into Vestibule.
- Imperforate Anus with Perineal Fistula — Rectum is abnormally opening into Skin.
Associated Conditions:
Anorectal Malformation has association with many conditions (VACTREL Anomalies). In a routine, we check all of them among these patients. These include:- Vertebral Anomalies
- Anorectal Malformation
- Cardiac Problems
- Tracheoesophageal atresia
- Renal problems
- Limb problems
Diagnosis of Anorectal Malformation:
We make the diagnosis of this condition on history and examination. After this, we advise some routine tests. These include X-ray of the tummy, Echocardiogram, X-ray of the back, and Ultrasound of the tummy.Treatment:
Treatment of this problem depends upon which type of problem the child is having and the child’s age. Usually, we follow this scheme: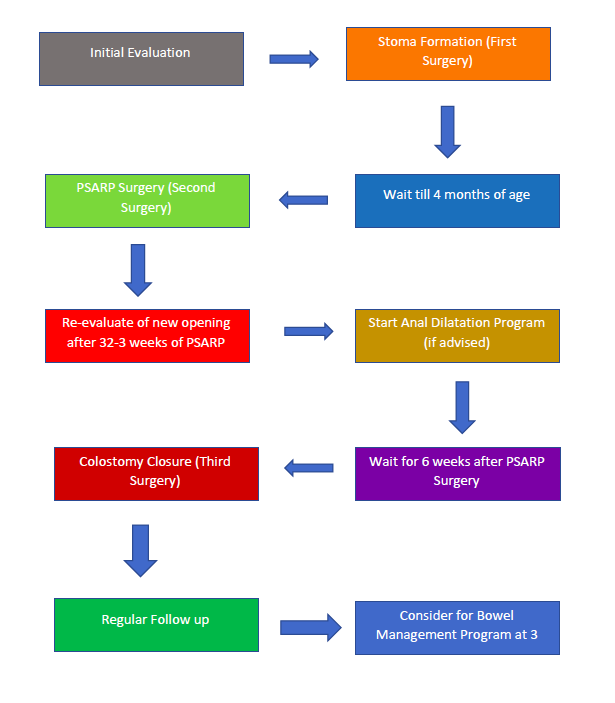 Most children with Anorectal Malformation present in the early days of life, and the first surgery (Colostomy)is done. Following that, all investigations are done, and then PSARP is done at 4 months of age. After that, the child is advised to start the Anal Dilatation Program. After 4-6 weeks of PSARP, the third surgery, Colostomy Reversal, is done. We keep the child in follow-up. At 3 years of age, the Bowel Management Program is started. If the problem of the child is of a mild type, in some cases, we may go for one-stage surgery. Sometimes, children present later in life at a few months of life; still we follow the same scheme. Schedule Colorectal Surgery
Most children with Anorectal Malformation present in the early days of life, and the first surgery (Colostomy)is done. Following that, all investigations are done, and then PSARP is done at 4 months of age. After that, the child is advised to start the Anal Dilatation Program. After 4-6 weeks of PSARP, the third surgery, Colostomy Reversal, is done. We keep the child in follow-up. At 3 years of age, the Bowel Management Program is started. If the problem of the child is of a mild type, in some cases, we may go for one-stage surgery. Sometimes, children present later in life at a few months of life; still we follow the same scheme. Schedule Colorectal Surgery